Neuroscience

Deep brain stimulation (DBS) for treatment-refractory psychiatric disorders has been gaining in popularity. The procedure involves neurosurgery to implant stimulating electrodes aimed at a target region inside the brain. It works using the same sort of pacemaker-like device used for DBS in Parkinson's disease, which has been remarkably successful at alleviating symptoms. DBS as a treatment for neurological disorders such as Parkinson's, primary generalised dystonia, atypical tremor syndromes, cluster headache, phantom limb pain, and epilepsy has been mostly unobjectionable.
However, the Neurological/Psychiatric Divide makes DBS for mental illnesses such as major depression and obsessive compulsive disorder more ethically problematic. A new paper in the Archives of General Psychiatry (Rabins et al., 2009)1 summarizes a consensus conference held on this and related issues (such as human subjects protection and the design of clinical trials). A list of 16 guidelines was issued, which included the following:
The topographical location of the nucleus accumbens in relation to other brain structures on a horizontal plane 3 mm below the AC-PC plane (Schlaepfer et al., 2007).
That protocol was designed to relieve anhedonia (inability to experience pleasure from normally pleasurable life events) in major depression. Why not stimulate the "pleasure center" when you're feeling blue? Extensive research in animals and humans has demonstrated "hedonic hot spots" (Pecina et al., 2006) [or "liking" of pleasant sensory experiences] in the NAcc that respond to food and pharmaceutical and financial and sexual rewards.
But what are the procedures for targeting the same region to reduce reward and pleasure? Well, we don't know from reading Heinze et al. (2009): "Details regarding the stimulation protocols in the different patients can be found elsewhere" [insert citation of an in press paper that is not online yet]. Details on the "clinical aspects" are pretty sparse and the focus is on the "basic science aspects" (electrophysiological recording and cognitive task performance to assess action monitoring and the salience of drug-related cues).
Was the DBS treatment effective? All patients had failed multiple detox treatments, withdrawal therapies, and drug trials (acamprosate). Until the other paper is published, we have only anecdotal reports in the Methods.
Footnotes
1 Guidelines were also published by the German Deep Brain Stimulation Association (Voges et al., 2009).
2 "A fourth had been implanted but electrodes had to be removed because of an infectious complication."
References

Heinze, H. et al. (2009). Counteracting incentive sensitization in severe alcohol dependence using deep brain stimulation of the nucleus accumbens: clinical and basic science aspects Frontiers in Human Neuroscience, 3. DOI: 10.3389/neuro.09.022.2009
Pecina S, Smith KS, Berridge KC. (2006). Hedonic hot spots in the brain. Neuroscientist 12:500-11.
Rabins, P. et al. (2009). Scientific and Ethical Issues Related to Deep Brain Stimulation for Disorders of Mood, Behavior, and Thought. Archives of General Psychiatry, 66 (9), 931-937.
Robinson TE, Berridge KC. (2008). Review. The incentive sensitization theory of addiction: some current issues. Philos Trans R. Soc Lond B Biol Sci. 363:3137-46.
Schlaepfer TE, Cohen MX, Frick C, Kosel M, Brodesser D, Axmacher N, Joe AY, Kreft M, Lenartz D, Sturm V. (2008). Deep Brain Stimulation to Reward Circuitry Alleviates Anhedonia in Refractory Major Depression. Neuropsychopharmacology 33:368–377.
- Deep Brain Stimulation For Bipolar Depression
The Melancholia of Kirsten Dunst and Lars von Trier “Gray wool, clinging to my legs, it's heavy to carry along” The disastrous wedding reception of the severely depressed Justine precedes the end of the world, depicted as a highly stylized and...
- Mania And Artistic 'surprise' Induced By Deep Brain Stimulation
Fig. 2 (Haq et al., 2010). A painting made following initial ALIC-NA [anterior limb of the internal capsule/nucleus accumbens] DBS activation. It was produced after a night-long effort and was described as a ‘surprise’ for the staff. The religious...
- Good News/bad News Update On Nucleus Accumbens Dbs For Treatment-resistant Depression
Taken from Fig. 1 (Bewernick et al., 2009). Hamilton Depression Rating Scale (PDF) over time. Two and a half years ago, The Neurocritic wrote about the very early results of deep brain stimulation (DBS) in the nucleus accumbens for severe, refractory...
- Great And Desperate Cures For Addiction
《Chinese Journal of Drug Dependence》1999-04 Does anyone know what aerosol bioelectricity is?? And why it might be used to treat heroin addiction? The entire literature seems to be in Chinese. I came across that particular paper while searching for...
- Nacc Localization For Dbs
The topographical location of the nucleus accumbens in relation to other brain structures on a horizontal plane 3 mm below the AC-PC plane (Schlaepfer et al., 2007). As the previous post discussed, the nucleus accumbens (NAcc) is an experimental target...
Neuroscience
Deep Brain Stimulation for Severe Alcoholism
Deep brain stimulation (DBS) for treatment-refractory psychiatric disorders has been gaining in popularity. The procedure involves neurosurgery to implant stimulating electrodes aimed at a target region inside the brain. It works using the same sort of pacemaker-like device used for DBS in Parkinson's disease, which has been remarkably successful at alleviating symptoms. DBS as a treatment for neurological disorders such as Parkinson's, primary generalised dystonia, atypical tremor syndromes, cluster headache, phantom limb pain, and epilepsy has been mostly unobjectionable.
However, the Neurological/Psychiatric Divide makes DBS for mental illnesses such as major depression and obsessive compulsive disorder more ethically problematic. A new paper in the Archives of General Psychiatry (Rabins et al., 2009)1 summarizes a consensus conference held on this and related issues (such as human subjects protection and the design of clinical trials). A list of 16 guidelines was issued, which included the following:
2. Deep brain stimulation for disorders of MBT [Mood, Behavior, and Thought] is at an early proof-of-principle stage and must be considered investigational. Currently, no single target has been validated or demonstrated to be superior to others in any disorder of MBT. Therefore, it is premature to rule out the study of new implantation sites that have a good scientific rationale...3. The comparative efficacy and safety of DBS vs other treatments, including ablative surgery, should be studied further. Such studies are ethical and scientifically necessary.4. Given its history, neurosurgical intervention for disorders of MBT is a socially and culturally sensitive area of research and practice. Therefore, DBS for disorders of MBT should be studied in carefully designed trials and should be performed only at expert centers that are participating in such trials and that adhere to the highest scientific, clinical, and ethical standards.. . .12. The consent process should include discussion of what is and is not known about long-term consequences of DBS. Potential adverse outcomes include potentially limiting participation in future research, inability to use certain other treatments, and an inability to undergo certain tests. ... Additionally, the consent process should state explicitly that, even with positive outcomes, DBS for disorders of MBT is unlikely by itself to improve all aspects of the individual's mood, function, and interpersonal relationships: DBS is only one aspect of a comprehensive treatment program.The specific indications mentioned by Rabins and his 18 co-authors were major depression, obsessive-compulsive disorder, and Tourette syndrome. Severe alcohol dependence was not included as one of the disorders. DBS for alcoholism sounds rather drastic, doesn't it? Nonetheless, a German research group led by Hans-Jochen Heinze (et al., 2009) was not deterred. They recently reported results from 3 male patients2 with severe and refractory alcohol dependence as part of a small clinical trial that will ultimately include 10 patients.
Inclusion criteria are: male gender, age 25–60 years, finished detoxification and subsequent period of abstinence of at least 2 weeks. Moreover, the patients are required to have demonstrated treatment failures of at least two inpatient programs of at least 6 month duration, failure of anti-craving substances (e.g., acamprosate, naltrexone), failure of community and self-help programs. ... Patients are excluded, if they meet any of the following criteria: seizures during the detoxification phase, high score on neuroticism scales, antisocial personality disorder, clinically significant impairments on a neuropsychological test battery Further exclusion criteria were circumscribed brain damage or marked atrophy on MRI, alcohol-related personality change, and use of additional addictive substances.The target region? The nucleus accumbens (NAcc), the “Universal Addiction Site” -- an oversimplification, they admit, but still, the NAcc is...
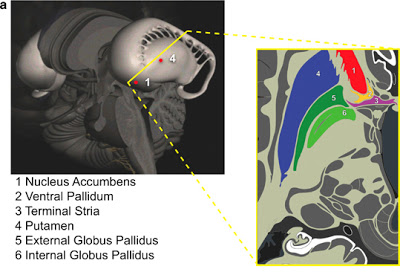
...a central place in orchestrating the events related to the “wanting” [Robinson & Berridge, 2008] of alcohol on the one hand and drug-induced neural sensitization on the other hand. Anatomically, the NAcc receives inputs from the prefrontal cortex on the one hand and limbic structures such as the hippocampus and amygdala on the other. This circuitry allows for the integration of contextual information arising from hippocampus and emotional information coming from the amygdala with cognitive information supplied by the PFC in the selection of goal-directed behaviors in general and behaviors related to drug “wanting” in particular, which is why the NAcc has been called a limbic-motor interface.Since anatomical information was not illustrated in the current paper, a figure from the earlier work of Schlaepfer et al., (2007) is presented below.
The topographical location of the nucleus accumbens in relation to other brain structures on a horizontal plane 3 mm below the AC-PC plane (Schlaepfer et al., 2007).
That protocol was designed to relieve anhedonia (inability to experience pleasure from normally pleasurable life events) in major depression. Why not stimulate the "pleasure center" when you're feeling blue? Extensive research in animals and humans has demonstrated "hedonic hot spots" (Pecina et al., 2006) [or "liking" of pleasant sensory experiences] in the NAcc that respond to food and pharmaceutical and financial and sexual rewards.
But what are the procedures for targeting the same region to reduce reward and pleasure? Well, we don't know from reading Heinze et al. (2009): "Details regarding the stimulation protocols in the different patients can be found elsewhere" [insert citation of an in press paper that is not online yet]. Details on the "clinical aspects" are pretty sparse and the focus is on the "basic science aspects" (electrophysiological recording and cognitive task performance to assess action monitoring and the salience of drug-related cues).
Was the DBS treatment effective? All patients had failed multiple detox treatments, withdrawal therapies, and drug trials (acamprosate). Until the other paper is published, we have only anecdotal reports in the Methods.
Patient HM (age 36) had started to drink alcohol at age 12 and had a family history of alcoholism (father and two uncles). ... The patient was implanted on October 5, 2007 and has been abstinent since then. There were no psychological changes after the operation. The patient reported to have no craving symptoms and that he is thus able to derive pleasure from daily activities of life. He has found a job and has established new social contacts.To be continued....
Patient GM (age 37) had started to drink alcohol at age 11 and had a positive family history (father, mother, several other relatives). ... Following the operation (January 13, 2008) this patient experienced a period of hypomania which stopped after stimulation parameters were changed. The patient has been abstinent since the operation and reports a complete reduction of his reaction to alcohol-related cues and craving.
Patient TM (age 40) had been alcohol-dependent since age 18 and had a positive family history (father). ... The patient was operated on September 13, 2007 and showed no psychological abnormalities in the postoperative period. He was fully abstinent until September 2008. Subsequently, he has experienced short periods of relapse of 1–2 weeks duration (10 weeks in the past 16 months). The patient remarked that he had never felt as good as currently and reported a considerable reduction in his reaction to alcohol-related cues.
Footnotes
1 Guidelines were also published by the German Deep Brain Stimulation Association (Voges et al., 2009).
2 "A fourth had been implanted but electrodes had to be removed because of an infectious complication."
References
Heinze, H. et al. (2009). Counteracting incentive sensitization in severe alcohol dependence using deep brain stimulation of the nucleus accumbens: clinical and basic science aspects Frontiers in Human Neuroscience, 3. DOI: 10.3389/neuro.09.022.2009
Pecina S, Smith KS, Berridge KC. (2006). Hedonic hot spots in the brain. Neuroscientist 12:500-11.
Rabins, P. et al. (2009). Scientific and Ethical Issues Related to Deep Brain Stimulation for Disorders of Mood, Behavior, and Thought. Archives of General Psychiatry, 66 (9), 931-937.
Robinson TE, Berridge KC. (2008). Review. The incentive sensitization theory of addiction: some current issues. Philos Trans R. Soc Lond B Biol Sci. 363:3137-46.
Schlaepfer TE, Cohen MX, Frick C, Kosel M, Brodesser D, Axmacher N, Joe AY, Kreft M, Lenartz D, Sturm V. (2008). Deep Brain Stimulation to Reward Circuitry Alleviates Anhedonia in Refractory Major Depression. Neuropsychopharmacology 33:368–377.
- Deep Brain Stimulation For Bipolar Depression
The Melancholia of Kirsten Dunst and Lars von Trier “Gray wool, clinging to my legs, it's heavy to carry along” The disastrous wedding reception of the severely depressed Justine precedes the end of the world, depicted as a highly stylized and...
- Mania And Artistic 'surprise' Induced By Deep Brain Stimulation
Fig. 2 (Haq et al., 2010). A painting made following initial ALIC-NA [anterior limb of the internal capsule/nucleus accumbens] DBS activation. It was produced after a night-long effort and was described as a ‘surprise’ for the staff. The religious...
- Good News/bad News Update On Nucleus Accumbens Dbs For Treatment-resistant Depression
Taken from Fig. 1 (Bewernick et al., 2009). Hamilton Depression Rating Scale (PDF) over time. Two and a half years ago, The Neurocritic wrote about the very early results of deep brain stimulation (DBS) in the nucleus accumbens for severe, refractory...
- Great And Desperate Cures For Addiction
《Chinese Journal of Drug Dependence》1999-04 Does anyone know what aerosol bioelectricity is?? And why it might be used to treat heroin addiction? The entire literature seems to be in Chinese. I came across that particular paper while searching for...
- Nacc Localization For Dbs
The topographical location of the nucleus accumbens in relation to other brain structures on a horizontal plane 3 mm below the AC-PC plane (Schlaepfer et al., 2007). As the previous post discussed, the nucleus accumbens (NAcc) is an experimental target...